Joraaver Chahal
Cadaver Dissection
Jul 01, 2025I had an amazing opportunity two weekends ago to travel to Charlotte, North Carolina and dissect a human cadaver under the guidance of experts at Experience Anatomy. The experience was rewarding and exhausting, the usual suspects in any time well spent.
Experience Anatomy’s promise was that any person who attends would get two full days with a human cadaver and would get to see everything, inside and out. The only asks were to come with one or two projects in mind to focus on, and the curiosity to absorb everything else.
I bought the ticket for about $1350 last year in September, before all my surgery issues. Afterwards, I didn’t think or do too much research. I just marked the date, populated a small todo list in the back of my mind, and moved on.
Last year, I began reading a book on the details of foot and ankle biomechanics (which you can glimpse in my notes), before I thought about finding a cadaver lab. While my study began as a simple fascination with my plantar fasciopathy after ACLR, I became engrossed with the literature and the science of the study as well, kicking off the question “is there a way to dissect a cadaver with no formal training?” My twin brother was able to while attending UC Berkeley, and I had always wished that I had that same opportunity at UCLA.
A week before the trip, I set up blocks of time to research my project: a deep focus on the effect of the posterior tibialis and flexor hallucis longus on the arch of the foot and how knee flexion affects the length tension relationship of those two muscles, and thus arch mechanics. This dissection would help me appreciate the nuance of tissue organization and the complex interconnectedness within the human body before I oversimplified it for for my project’s needs. “All models are false; some are useful” becomes much easier to grasp when you get to see the full system the model is trying to abstract. The week’s preparation was spent looking at a copy of Grant’s Dissector and taking notes about how to dissect the leg, or shank, depending on what sources you’ve learnt your terminology from, and the foot. Because I didn’t want to buy the book, I checked out an old edition from the Open Library. I am relieved to tell you that the method of dissecting the calf hasn’t really changed in the almost thirty years since the publication of my edition of Grant’s Dissector and that someone brought a much more recent copy to the dissection so we could take off our gloves and flip through it when confused or unsure, which I took great advantage of.
I received an email the day before the event informing us of a location change because the lab had been double booked. We were to perform day one’s dissection in the Sheraton Hotel. You can imagine my disbelief. How do you even prepare a dissection at a hotel? She assured us we would still have a fabulous time, with an added scenery change. Exquisite.
Category: Just Medical Things, for $1000. When you enter the lobby of a hotel, looking for a cadaver dissection event, what do you look for?
What is “a bunch of confused women in scrubs?”
Correct!
I joined the crowd in my old shirt and jeans and we found our way without making too much of a scene. I forget how much healthcare is a female dominated field. In our group of twenty-one students, only three were men. As for professions, there were massage therapists, physician assistants, yoga instructors, acupuncturists, physical therapists, personal trainers, aspiring medical students going to college, and of course, me, a software engineer. Oh, and a high schooler who had already been doing dissections for over a year. She was only here to do a full dissection of the hand. Diverse crowd.

The Dissection
The cadavers were all face down when we entered. The instructors did an initial demonstration of scoring, incising, and layer identifying on the upper back for about ten minutes. We were going to tackle just the posterior aspect of the body for most of today, and then we would decide to flip the body based on our progress. After that instruction, we were let loose.
You could instantly tell who was comfortable going in and who was hesitant. Where do you make the first cut? How long? What if you go too deep? Obviously points we had talked about, but if you’ve never opened a body before, that first cut is still a daunting task.
Nonetheless, we cut. Ideally, we all cut broad and shallow, layer by layer. Everyone took a distinct part of the body, seven people to a body, three bodies.
The first thing you appreciate is the difference in body fat between the sections of the body and across bodies. The back can store a lot of fat; the calf, far less. Then, muscle thickness and morphology can be wildly different from person to person. If all you think about are muscular, lean bodies, you can imagine how incorrect your mental model will be for what’s going on in the body of the average sixty-five year old American woman.
The layers aren’t always clean. Fat can infiltrate the deeper layers. Muscles can adhere to each other and to the fascia. Differentiating the soleus from the gastrocnemius the way diagrams suggest they exist certainly isn’t easy.
If you are trying to study the human body, it doesn’t help to just blindly slice through its parts. Sadly, I severed the tendon of the semitendinosus when trying to expose the popliteal fossa and find the origins of the gastrocnemius. Some worried I severed the sciatic nerve. How could they assume something so sinister of me? They barely knew me!
All the more reason to question me, I suppose.
Everything sticks together. Fascia covers everything. Outlines everything. Envelopes everything. Yet, what needs to glide, glides. The fascia develops in a way to support the movement needs of the tissue it interacts with. Single and multi-plane movement of the muscles, enlarging and shrinking of the heart, or preventing movement at all when necessary.
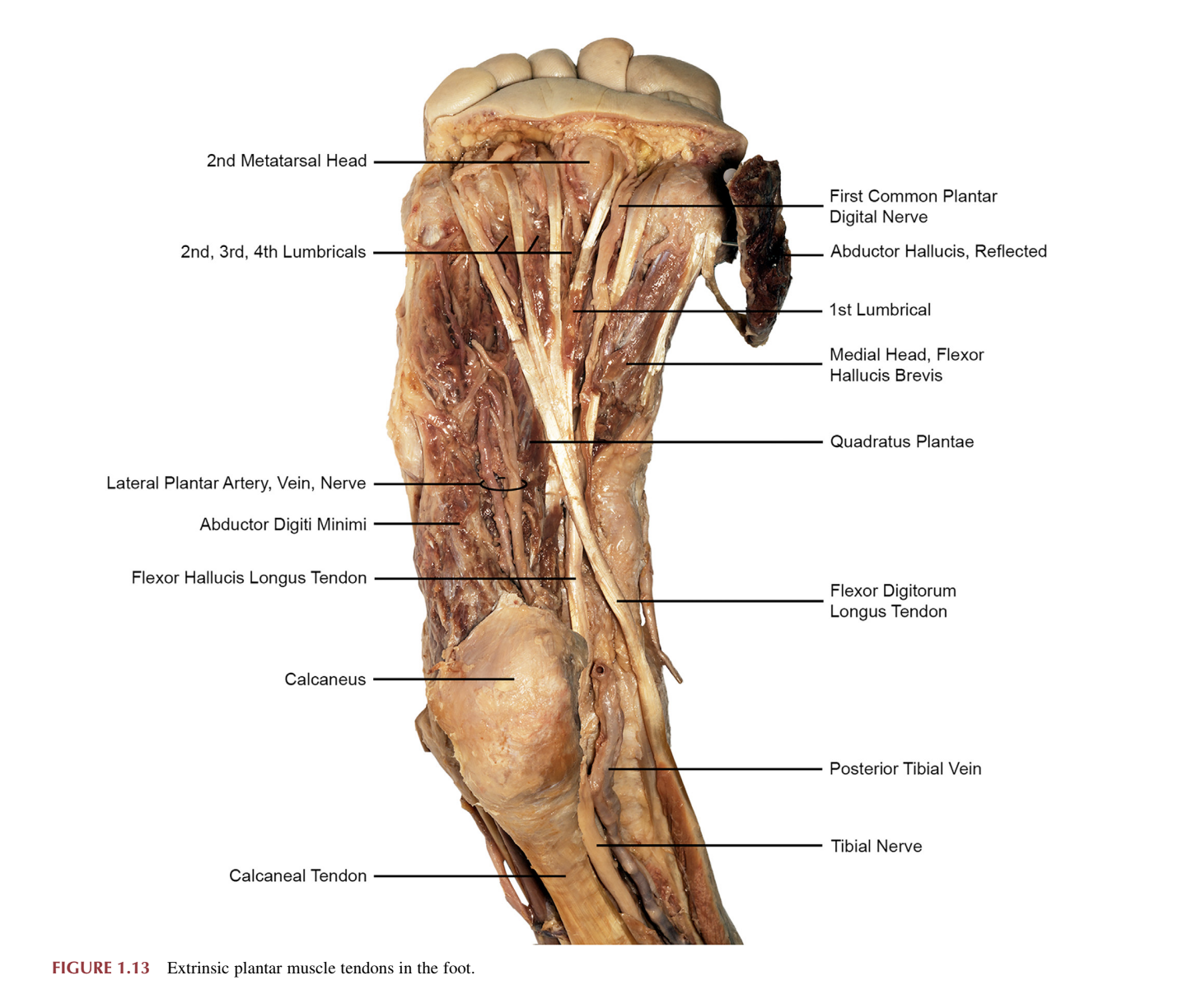
Case in point, and eye opening for me, were the intricacies of the fascia as I dissected the sole of the foot to uncover the insertion of the flexor hallucis longus (henceforth FHL) into the first metatarsal. If I tugged on the tendon from the base of the foot, flexion of the great toe was obvious. However, if I reached into the calf and tugged on the muscle belly of the FHL, the smaller digits flexed alongside the great toe, but to a lesser degree. The flexor digitorum longus (FDL) and FHL run through the same retinaculum and overall fascia that holds the tendons in place. Does that mean you can’t train the FHL independently? Not quite. After all, I’m manipulating a dead body. Nothing at all like a live subject. All that matters regarding exercise prescription is if you can stimulate the desired muscle and how important other muscle activation is to you. If you can isolate, isolate. If you can’t, don’t stress. In fact, understanding that the fascia also adapts to the ways we move is quintessential to moving well in a variety of domains that require speed, not just force, and is often a neglected aspect of inexperienced movement practitioners’ training plans.
After the lunch break on the second day, I stopped all dissection for two good reasons: because I finished my project, and because I had no clue how to handle the internal organs, let alone what to look for. It was magnificent, watching the experts swiftly but accurately open, identify, and maneuver the internals of the body. However, understanding what I was looking at was a different story. In much the same way my mental model for musculoskeletal reasoning was off, the difference between what the organs looked like in my books versus what they were like in the pathological case was drastic. The woman our team was dissecting died of liver failure, so her liver was pink and hard, almost petrified. We had to wait for one of the other teams to open up the abdomen before seeing what a normal liver should look like. Her spleen was also swollen and black, which is definitely not normal. One person passed away due to COPD (chronic obstructive pulmonary disease), so that team walked around the room to take a quick peek at what a set of normal lungs, instead of a set with black lungs and collapsed alveoli. The third person passed away because of heart failure, making for an interesting dissection. He had a bypass surgery done before he passed, so not only could we observe the staples on the chest where the surgery was done, but also the stitches in the calf where his saphenous vein was taken and the stitch on his heart where he had the bypass done.
The dissection of the body ended with a full evisceration of the internal organs. That meant breaking the ribs, accessing the esophagus, cutting all the way through to the front of the spine, and slowly cutting away at all the fascia that holds the internal organs in place, eventually pulling out the whole system as one intact group, and laying it on the table. Again, I cannot overstate how much confidence these experts displayed while cutting. The one I watched do the first evisceration moved at full speed while admitting her fears at having possibly cut the psoas where it originates along the spine. She, in fact, did not.
After a nice midafternoon break, the last task took place on the body we thought had the best preservation: a craniotomy. The bone saw whirring, all the dust flying in the air, and the eventual removal of the top of the skull made for a morbid spectacle. Unfortunately, the embalming wasn’t good enough to hold the structure of the brain in place, and as soon as the experts attempted to pick up the brain and place it on the table, it turned to turn to mush. The instructor did her best to point out the structures within the brain, but it was a short-lived attempt, and so the remaining minutes were spent looking at the structures of the skull, now visible because the brain was gone.
To finish my dissection, I walked back over to my cadaver and, after getting clearance, snipped the ACL and performed a nice, easy, Lachman test. Ah, to feel the instability of the knee after a fresh ACL tear.
The Experience
I would be remiss to discuss my trip purely in terms of organs, muscles, tendons, ligaments, bones, nerves, arteries, and veins. Make no mistake, my primary intent was intellectual curiosity. But as always, it is the people who turned it into something more.
The dissection brought out the nerd in everyone. A safer space could not have existed for these folks to make both respectful and outright heinous jokes. Just so you understand how comfortable people felt, allow me to regale you with the comedy in question.
Around an hour or two after starting our dissections, I walked over to another table to inspect their cadaver’s left popliteal fossa (back of the knee), which that team had done a better job of exposing. As I hovered to observe, one woman swiftly handed me a small, purple, globular thing to hold. She told me to squeeze it. Get a feel for it. I said sure, but what on earth is this? “His testes!” she said, smiling brightly. Everyone else at the table laughed. I laughed lightly.
On day two, in the morning, we removed the right breast of the woman my team was working on. We passed it around to get a feel for breast tissue versus the mammary glands. I kid you not, as soon as it landed in my hands and I started feeling it, a woman on my team said “I bet breasts are gonna feel a whole lot different the next time you touch one!” It’s a good thing my sense of shame left me somewhere in childhood, because another man in my place would have been absolutely mortified.
Comedy aside, during lunch on the cloudy but humid second day, one instructor brought up the idea of the spirits of the bodies, and whether we felt their presence. The intersection of beliefs present is not something I thought we would discuss, but I suppose the very practice of dissecting bodies started in the realm of pure sacrilege, and it is thanks to those people continually progressing the practice that it has become the norm, allowing all beliefs to be present while still examining the science. I told my colleagues at the table that while I don’t feel any spirits, I do feel the emotional anguish and turmoil they may have felt regarding their surgeries and what the recovery must have been like.
Now is the proper time to make a nuanced point. A reflection of my previous statement, really. I remind myself that I simply cannot know how they handled it. I can relate to the initial pain, sure. But the apprehension of surgery, the people it would affect, or the difficulty of the rehab? At this point I’m just projecting. We cannot truly know without asking. And even when we ask, we cannot know unless they are willing to tell, and tell everything. Choosing to sympathize is okay, but feeling powerful emotions for narratives that exist only in your head, often translating into extolled behaviors that nobody asked for? Might as well live in a fairy tale.
On a separate note, because I was the only student doing a deep dive of the foot, I had a unique chance to show and teach others who were taking a break from their cadaver to look at my team’s cadaver. I have a funny memory of three students leaning really far over to look at the weirdly oriented foot I was working on as I explained each layer of the sole. It reminded me how much being able to teach well is a marker of expertise, and finding a small but focused group of students to do it among, from student to student, was quite the gift.
Wrap Up
Unfortunately, I don’t have many pictures to share of the experience. We weren’t allowed to take pictures during the dissection, for obvious reasons, but I have a pretty cool one in their lecture area:

I now possess a much stronger visualization of the inside of the flesh bag we move around in every day, and am extremely thankful to the folks at Experience Anatomy for the opportunity.
A reference popped into my head when I wrote down “flesh bag” but I didn’t know how to tie it nicely into my conclusion. So you get my straightforward take.
Your skin is a bag, of sorts. Taut in some places, loose in others. Gets looser over time. The term reminds me of the short story Skeleton by Ray Bradbury.
Stay taut flesh bags.
#technical #rehab #injury